Keywords: cult – 25 results, 'emotional contraction'(s) – 15 results,
Emotional Health in the Age of Disconnection
Perspectives on emotional integration and holistic psychiatry.

MAY 24, 2023
217
9
Many people believe the most significant issues facing the Western World are emotional in nature (e.g., anxiety is often termed the disease of the modern age). In turn, a common observation is how often the emotional patterns individuals carry end up controlling their lives (frequently causing them to make terrible decisions) and continually making it a miserable life to live.
I believe all of this arises from a few key things:
•Our culture has a misguided understanding of productively engaging with one’s emotions.
•Our economy depends upon systemic emotional dysfunction existing in the population.
•The medical field has been incentivized not to explore effective treatments for emotional conditions.
•Our modern society and environment are not conducive to mental health.
Because of the magnitude of this problem, many have adopted the perspective that unresolved emotional conflicts, past traumas, and psychiatric illnesses are the root cause of all diseases. While I have seen numerous instances where this was the case, I have also seen many patients who were given that assessment, did not improve from treatments for it, and instead had a completely different physical issue that needed to be treated for their recovery. More importantly, I have lost count of how many different (and widely promoted) approaches I have seen for addressing emotional issues. In most (but not all) cases, these approaches fail to do very much, which has created a massive industry of providing endless mental health support to those requiring it.
Because of the magnitude of this problem, even if I somehow knew all there was to know about it (which I don’t), I would not be able to do it justice with an entire book, let alone a single article. For that reason, I will have to exclude a wide variety of topics that deserve mention and instead focus on the ones I believe to be both important and largely unrecognized.
The Forgotten Side of Medicine is a reader-supported publication. To receive new posts and support my work, please consider becoming a free or paid subscriber.
Subscribed
Marketing Economies
To get individuals to buy something, typically one of two things needs to be done (assuming you don’t, for example, mandate a dangerous and ineffective product no one wants to receive):
•A good case needs to be made for the product is necessary to the buyer and can provide a value greater than its purchase cost.
•The product is sold based on emotional appeal rather than its intrinsic value.
Since the 1970s [this date was my best guess but may be incorrect], our economy has gradually transitioned from selling products based on their merits to selling based on an emotional appeal. This is because most of the population has a stronger response to this type of advertising (the broad implications of which will be discussed in an upcoming article) and because you can sell an unlimited number of things for emotional reasons. In contrast, the utility of many products can quickly evaporate after a sufficient number of purchases, thereby making it very challenging to sustain sales indefinitely if a product is marketed solely on its merits.
Almost all emotional marketing follows a straightforward formula:
1. Make the watcher feel bad (e.g., envious,
insecure, or self-loathing).
2. Present the product as the solution to those
negative feelings.
There are a few significant consequences of this:
First, this process (needing a product to alleviate emotional discomfort) is not a good way to handle difficult emotional experiences. As a result, individuals raised within a deluge of toxic marketing will most likely have numerous dysfunctional emotional coping mechanisms.
The second is that it requires the population to be kept in a constant state of negative emotions and emotional dysfunction (as emotionally healthy individuals are much less susceptible to emotional marketing). This kills any societal incentive to address the problem, and many other industries instead piggyback on it. For example, most news is designed to create negative emotions inside you (so you will be hooked to the station), rather than covering many of the positive stories that are constantly happening around us and creating a positive effect on the audience.
Note: this is why numerous integrative doctors over the decades have said one of the best things you can do for your health is to ignore the news completely. This advice is particularly concerning because as the years have passed, the media has gotten much better at agitating its viewers, and the news those past doctors warned against was relatively benign compared to much of what is aired now.
The third is that this marketing disproportionately targets women and gives them an almost uncountable number of ways to hate themselves on a very deep level so that they will continually buy products aimed at temporarily appeasing those feelings. Unless you are a woman who grew up in America, it is so difficult to appreciate just how pervasive this destructive marketing is and what it does to your sense of self. My own experience has been that it is exceedingly rare to find a man who gets this unless they work in marketing, and doing that to America is part of their job.
Healthy Emotional Coping Habits
The fundamental error underlying our culture’s concept of emotions is that they are neuronal impulses generated within the brain that are no different from thoughts. This gives rise to the belief they should be viewed as thoughts to be brought under control with other thoughts.
In reality, emotions are one of the many types of flows that run through your body. If they are engaged for what they are rather than being viewed as an abstract thought, having a harmonious and healthy relationship with them becomes possible. Unfortunately, while this is simple—it is almost never taught in our culture.
I feel incredibly fortunate to have had a spiritual teacher tell me at a young age:
You can’t think your way out of difficult emotions. All that can ever accomplish is to feed the energy underlying the emotion and prolong your suffering.
I consider this to be one of the most impactful pieces of advice I ever received, and I often wonder where I would have ended up had I not heard it. Unfortunately, a significant portion of the massive mental “health” industry revolves around thinking your way out of emotional pain, and I long ago lost count of the people I had met who had spent decades in therapy without it doing anything for them.
Many different holistic diagnostic models (e.g., Herrings Law of Cure from homeopathy) believe that pathogenic factors enter the body from the surface, become more chronic and severe as they penetrate deeper into the body, and that treatment should always aim to expel those conditions to the exterior instead. I endorse this model, and would argue one of the clearest demonstrations of it was the reactions[i] to the catastrophic smallpox vaccine. Unfortunately, modern medicine instead seeks to do the opposite by suppressing the symptoms that emerge when a pathogenic factor arrives at the surface (e.g., a fever or a rash), and this, I believe, is one of the core reasons for why so many chronic illnesses exist in our society.
Herring’s law of cure also describes what is necessary for having a healthy relationship with your emotions. When an emotion occurs, you have two choices. You can feel it, fully accept it, relax to its presence, express it, and let it pass out of you, never to trouble you again. Or, you can question the emotion, reflexively restrain expressing it, withdraw from it, and let it lodge inside of you, with the deeper it lodges, the greater an effect it has on the rest of your life.
Note: there are countless cases of individuals placed on SSRI antidepressants because they have dysfunctional situations at home (which feeling depression or anguish towards is a normal and healthy reaction towards). They often report going through the dysfunctional dynamics for years in an emotional daze before eventually quitting the SSRI and regretting how many years of their life they wasted because of the medication.
The clearest examples I have seen showing the relationship between SSRIs suppressing emotions and Herring’s law of cure occurred in individuals who (for questionable reasons—e.g., tolerable stress at work) were put on an SSRI and later violently killed someone they loved dearly. When I put together a compilation of the extensive evidence demonstrating that this happens and the SSRI industry is fully aware of it, I discovered cases of individuals who, prior to turning violently psychotic, externally, looked much calmer (thus making those around them believe the drug was finally “working”) but internally they were dramatically more unstable.
Many things make the method I advocate for quite challenging. The more intense an emotion is, the harder it is to relax into it, our society habitually conditions us to deny and withdraw from our emotions (as experiencing or showing them is viewed as something to be ashamed of), it can initially be difficult to authentically express an emotion in a calm and non-confrontational matter, and most importantly, almost every single resource we have teaches us to intellectualize our emotions rather than feel them.
This problem is also not unique to the Western World. Within Buddhism throughout Asia, for example, one of the central beliefs said throughout the scriptures is that a Buddha (holy being) perceives reality without attachment and that attachment is the root of suffering. In turn, there are three different ways those beliefs can be interpreted:
1. When you achieve a high level of spiritual development, the way you perceive reality changes, and many things you previously took so seriously, or your mind grasped onto instead fade away into emptiness.
2. Individuals with excessive attachments to things (or events) often lead miserable lives. When you recognize this quality in someone else, you may want to advise them to consider the Buddhist path as that will reduce the suffering in their life.
3. Buddha commanded us not to have any attachments. Furthermore, since the only meaning of life is to become enlightened, and becoming enlightened is a result of us discarding all attachments, we must collectively force ourselves to reject any possible attachment to anything.
1. I believe the first interpretation is accurate,
2. I periodically see cases where the second holds true, and
3. I firmly believe the third is entirely wrong.
However, the third interpretation is quite common (especially in Buddhist organizations that are more dogmatic or cult-like), and I constantly meet people I believe have essentially developed a mental illness from following it and suffered for years because of it.
To be more specific, I often observe these types of Buddhists habitually suppress their emotions (frequently being highly conflicted for doing so), abandon the human connections in their lives which gave them meaning, and engage in something no different from body dysmorphia where they view each part of their body (and bodies of the opposite sex) as disgusting. All of these behaviors are done so that they “lose their attachment” to things people are commonly attached to (e.g., your feelings, your body, or intimacy and connection with another human), in the belief that will move them towards enlightenment. Sadly it typically accomplishes the opposite.
Note: I mean no disrespect to the Buddhist tradition (rather, I deeply admire it). It’s just that, like every other large group, it has factions that do not pursue the ideology in the healthiest manner.
Emotional Contractions[ii]
Since I was a child, I noticed that when people said things, especially if they expressed their emotions in a restrained way, I would often feel something within their bodies tighten or contract. As time passed, I noticed many people with habitual emotional patterns (that were often unpleasant to deal with) would have the same places in their body contract each time the pattern occurred. Thus, gradually, I began to view the emotional pattern as a result of the pre-existing contraction rather than whatever story existed to explain their pattern.
Note: many consider What Every BODY is Saying: An Ex-FBI Agent's Guide to Speed-Reading People one of the best books on learning body language. What I found most intriguing about the author's approach (based around assessing comfort and discomfort) is that almost every non-verbal expression I consider equivalent to contracting the body he classified as indicating distress or discomfort, while all those doing the opposite he classified as indicating comfort.
My observations were by no means unique. One of the earliest Western pioneers of this subject was Freud’s contemporary Wilhelm Reich, who made numerous fascinating discoveries (I hope to cover them in the future), including a psychotherapy system still practiced worldwide. A key component of his approach was addressing what Reich termed armoring:
Armor is a metaphor referring to the muscular spasms, decreased motility, postural misalignments, and character attitudes which an individual develops that act as a defense against the breakthrough of unwanted or intolerable feelings, sensations, emotions, or experience. Muscular armor serves, mostly, as a defense against anxiety, anger, fear, and sexual excitation. Character armor leads to emotional rigidity, poor contact with others, and a feeling of ‘deadness.’ With armor in place, the conscious control no longer has to actively defend against certain impulses or desires. As tenacious as psychological defenses tend to be, they can still slip or be overwhelmed at times, but armor tends to be 'always on.'
Note: While I cannot prove it, since many people I’ve spoken to also feel emotional contractions, I strongly suspect Reich’s focus on “armoring” arose from him feeling the contractions associated with its occurrence. Recognizing physical and, especially, emotional contractions is immensely valuable in human relationships because they can often identify problems under the surface the other party will avoid mentioning until it is too late to salvage the relationship. For example, throughout my life, I have seen more cases than I can count of couples who loudly proclaimed how deep their love was for each other (all the while displaying emotional contractions suggesting otherwise) and shortly after separated on acrimonious terms.
Another well-known advocate of the emotional contraction model, Joe Sarno MD, theorized that a significant amount of back pain resulted from unresolved emotional conflicts creating chronic tension (contractions) of the muscles in the back, which in turn gave rise to back pain. Many people have had a great deal of success with his approach (Sarno termed the condition tension myositis syndrome), and while the medical community does not yet accept it, there are a few studies showing Sarno’s method works.
My own observations of the consistent patterns I saw in emotional contractions eventually prompted me to also research numerous spiritual traditions, where I found that the patterns of emotional contractions I observed overlapped with many of their maps of the human body, mind, and spirit. These systems view the body, mind, and spirit as an interrelated unit where each shares similar behaviors to the others (e.g., a physical contraction such as clenching your fist for a prolonged period is ultimately not all that different from an emotional contraction or a mental contraction).
Note: As the years go by, I see more and more connections between the body, mind, and spirit, and in many complex cases, I've found the patient cannot recover unless all three are treated as an inseparable unit. Unfortunately, this is an incredibly complex subject, and even after decades of working with it, I still often have no idea what I am doing when I interface with it during a patient encounter.
When I entered medical school, my attention started being drawn much more to those contractions, and I began to notice how often people would close something inside themselves down when they were confronted with evidence that challenged their pre-existing dogmas. For example, I had a few cases where a supervising doctor was confronted with evidence he or she had medically injured a patient. Once this happened, something in their heart or brain closed down, and that was immediately followed by the doctor disassociating into a trance where they gaslighted the patient and diverted the patient's focus from the medical injury.
"You can't rationalize facts to someone whose position is based on emotion" -Ed Dowd
Although this topic is a bit esoteric, I feel it is important to share for a few reasons.
The first one is that I (and colleagues) often find the reason that people refuse to listen to facts that challenge their cherished beliefs is because of those habitual contractions. So, as the years have passed, my focus in debating people has gone from the facts themselves to how I interact with their emotional contractions. While challenging, this is a much more effective way to get through to people.
Note: I (and many of my colleagues) have learned from experience this approach must be done in moderation because if deeply entrenched patterns shift too quickly, it can be too much for the individual to handle.
The second one is that when I can tell someone's behavior is based on emotion rather than facts (e.g., for a patient with a specific issue that says they “want” help with it but is simultaneously constantly self-sabotaging themselves), I find one of the most effective ways to help them is to bring their attention to the contraction underlying the dysfunctional emotion. Often people aren't even aware of it until you point it out, but once you do, their perspective broadens, they feel seen (which is very important in the doctor-patient interaction), and they become much more mindful in not recreating their pattern.
Note: various approaches have been developed for addressing the contractions within the body that give rise to those dysfunctional emotions. In general, instructing the patient to become aware of that contraction and relax or breathe into it to begin fostering body integration helps. Beyond that, therapeutic efficacy highly varies depending on the practitioner (many provide minimal benefit, while some are extraordinary).
The final one is how often people lie to themselves. I believe this is due to how much we in America (much like the dogmatic Buddhists) suppress our emotions, as this results in many of those emotions becoming ingrained within our unconsciousness and causing us to reflexively engage in behaviors we are internally conflicted over and disagree with. The degree to which things patterned into the unconscious mind influences human beings is incredible and, quite frankly difficult to believe unless you have witnessed it firsthand in a large number of people.
Throughout my life, I have felt very strongly about respecting people's free will and autonomy—which has been quite challenging when I've had to watch people I wished the best for destroy their lives because they failed to follow our advice. Although I held to this principle for a long time, a few people I'd worked with who were trapped in cults changed my perspective on this issue.
That was because, from the pattern of their contractions, I realized that what they said they wanted (to devote their lives to the destructive cult) was only stated on a superficial level because it was in complete conflict with much of their body, mind, and spirit. After I made a choice not to interfere with the "free will" of one cult victim (and then watched the expected unfortunate outcome occur), the next time I ran into the situation, I rationalized taking a much more active role in their cult intervention was ethically permissible because "being in the cult was not that individuals 'free will' and I was only helping to reconnect them with their free will." When it was all said and done, the cult victim thanked me profusely, saying that the cult had stolen their free will and it would have been terrible had they stayed.
At this point, I am still not sure where it is appropriate to draw the line with respecting someone's autonomy, but I share this to illustrate just how complex emotional contractions and suppressing your true feelings can make life.
Drugs and Alcohol
Since our culture does not teach us practical ways of coping with emotional difficulties (particularly emotional pain), one of the most common approaches people adopt is self-medicating with substances. I find this particularly tragic because everyone knows this is not a good approach, yet the media continually promotes it because so much money is made from it.
Because of this, much in the same way the pharmaceutical industry has, through decades of work, successfully created a "pill culture" where people pop pills rather than taking responsibility for their health, we also have a "drug culture" for mental health. In the case of substances, this is a real shame because using the substance to shield oneself from emotional discomfort takes away the individual's ability to develop mature coping skills for emotional distress. For instance, I have seen many cases where patients who began smoking marijuana in childhood to deal with emotional pain never stopped using it for that purpose, and by adulthood were effectively crippled emotionally as they had immense difficulty dealing with any type of stressful situation.
Generally speaking, the substances used for this purpose act similarly; they either suppress or disconnect the user from their emotional discomfort (along with many other aspects of their body, mind, and spirit). By doing so, the challenging emotion lodges deeper within them and creates more severe issues, which sadly, then "requires" more self-medication. When you also consider that the media primes us to crave temporary spikes of dopamine and the addictive nature of many of these substances, the problem quickly compounds itself, and not surprisingly, addicts are sadly quite common.
Although this is probably ultimately not possible to determine, my general impression is that people are much more susceptible to getting addicted to substances now than in the past (e.g., many of the current illegal drugs used to be freely handed out at pharmacies).
Note: if you study the history of opium (e.g., the opium wars), it is a drug that potentially refutes this assessment.
As best as I can tell, two factors account for this:
•First, many things that previously gave us purpose and meaning have been lost. Because of this, the high from a substance that can fill that void becomes almost irresistible since it fulfills the vital need every human being has for an existential purpose (this will be covered more in an upcoming article).
•Secondly, the digital age has disconnected us from our bodies because it requires us to be in our heads and minimize our engagement with the physical world.
This becomes a severe problem because much of what fundamentally makes people "happy" (and many people spend their lives searching for it) is a product of being connected to yourself (particularly your body) and our world—which is very different from living in your mind and constantly disassociating from everything.
Since people don't have that intrinsic connection, they instead search for fulfillment in things like substances or gravitate toward ideologies (like the nihilistic sects of Buddhism mentioned above) that provide an excuse to withdraw from the parts of the world they can't connect to. Additionally, the more disconnected people are from their bodies, the more external influences (e.g., a stressful situation) will destabilize them, and the less they can recognize what is occurring when it happens (thus often making the emotional destabilization feel like an overpowering situation they are powerless against).
Note: While I cannot prove this, I believe this shift away from reality has been done so that "wealth" can be created from nothing (e.g., because people will pay for "gold" on online video games that is earned by completing repetitive tasks, there have been numerous cases of what is essentially slave labor being performed to obtain it). This then provides a way for the elite to continue to hoard our limited resources while providing the rest of the population with the illusion of "wealth." Since this newfound wealth is an illusion, trying to possess it (in the same way many covet "rare" knowledge) is not good for the human soul and seems to make us be further and further disconnected from reality.
Lastly, Gabor Maté, a well-known Canadian psychiatrist in his book In the Realm of Hungry Ghosts: Close Encounters with Addiction, shared one of the more interesting perspectives on drug addiction. Maté made a strong case (with the evidence to support it) that drug addiction, especially towards stimulants (e.g., meth or cocaine), often occurs due to childhood trauma that rewired the nervous system's sensitivity and caused the individual to lose the ability to feel loved. Only while they are high on those drugs can they experience that feeling. As many who have had to deal with a drug addict they are close to can attest, it is incredibly challenging to maintain compassion for the addict due to how far they will go just to keep on getting high. For anyone in that situation, I think Maté's book provides one of the most helpful perspectives I have seen for individuals trying to maintain compassion in those situations.
Psychedelics
While I have never gone down that road, quite a few of my friends have become very committed to using almost every psychedelic in existence for self-development and resolving psychiatric issues such as emotional trauma, and they regularly share their experiences with me. As someone who is frequently around psychedelics but has no personal investment in them, I feel I can offer one of the more objective perspectives on this subject.
In general, I have found that people who regularly use psychedelics for personal growth or healing tend to believe they significantly benefitted from doing so (and develop egos over the experiences they had on them). However, other than making them more open to spiritual perspectives, it is quite rare for me to encounter someone who appears to significantly have benefitted from them (e.g., people talk about how they resolved their emotional traumas and dysfunctions but often continue to display them identically to how they did before their psychedelic journey).
In my eyes, a key misunderstanding with psychedelics is that most of them are not inherently healing but rather function by significantly increasing the brain's neuroplasticity. Thus, if someone on a psychedelic works with an experienced therapist, they can achieve profound benefits, but if the individual's focus is not on effectively resolving their emotional trauma (which rarely happens without a skilled therapist), the increased neuroplasticity is wasted, and in many cases detrimental if the focus at the time is instead on something dysfunctional.
Although I have seen many things go awry with psychedelic use, I also fully recognize their value—I have seen some remarkable things with them. People I knew who did LSD psychotherapy decades ago (before it got outlawed) for example had incredible results with lifelong alcoholics (a condition that is exceptionally difficult to treat).
Similarly, I know people who have been able to restore neurological function they lost after a stroke during a guided session of psilocybin and LSD. Andrew Weil, MD, shared one of my favorite examples of [what] LSD can do on Joe Rogan:
While on LSD, a cat jumped in Weil’s lap and, at that moment he was able to
make his lifelong allergy to cats permanently disappear.
Currently, I've seen the best results from ketamine being used therapeutically in guided sessions with a psychiatrist (it can sometimes resolve a wide range of issues). For individual use, many people have told me micro-dosing LSD or psilocybin greatly aids their creativity (with the people I knew, LSD used to be more commonly used for that purpose, now psilocybin seems to be more the preferred choice), and I have not yet run across someone with an adverse experience from this practice. Lastly, individual psychedelic experiences frequently create a very positive outlook on the world for the user. Still, this benefit only requires a few sessions to achieve. It is pretty rare (unless the experience occurred under the supervision of a therapist) that the user will not continue to use psychedelics recreationally after that time. This matters because at that point, I have frequently seen the initial benefits reverse.
This is a very superficial review of an immensely complex subject. For example, I did not discuss ayahuasca (which is very popular these days and, like the other psychedelics, really needs to be done under the supervision of the right person) or DMT (and the remarkable book written by the physician who was allowed to research DMT—and for which the documentary is one of the most streamed documentaries on Netflix). Similarly, I did not discuss how MDMA (ecstasy) is being researched as a treatment for PTSD.
I believe that psychedelics have a lot of potential to resolve many of the issues psychiatry presently struggles with (and a few of my psychiatrist colleagues are very committed to moving their profession in that direction). However, it will take a while for the research to be developed to make this happen (it is a relatively recent development that research in this area stopped being taboo), so there is still much to discover.
If you decide to do this route, I would strongly advise doing it with a psychiatrist who has earned a reputation for being experienced with psychedelic-guided therapy. Furthermore, a lot of things can go wrong with them (especially LSD), and you need to be honest with yourselves about those risks before you choose to go down that route.
Conventional Psychiatry
Many consider anxiety to be the disease of the modern age (e.g., since modern marketing aims to condition you to be trapped by the expectation of getting an emotionally needed product in the future, that conditioning makes it very difficult for you to ever be content in the present instead of constantly being worried about what could happen in the future).
Once you are a healthcare provider, it becomes astounding to see just how many people are afflicted with crippling anxiety. For example, at this point in time, 19.1% of US adults had an anxiety disorder in the past year, 31.1% will at some point in their lives, and 4.7% suffer from regular feelings of depression. Similarly, consider the results of a recent survey:
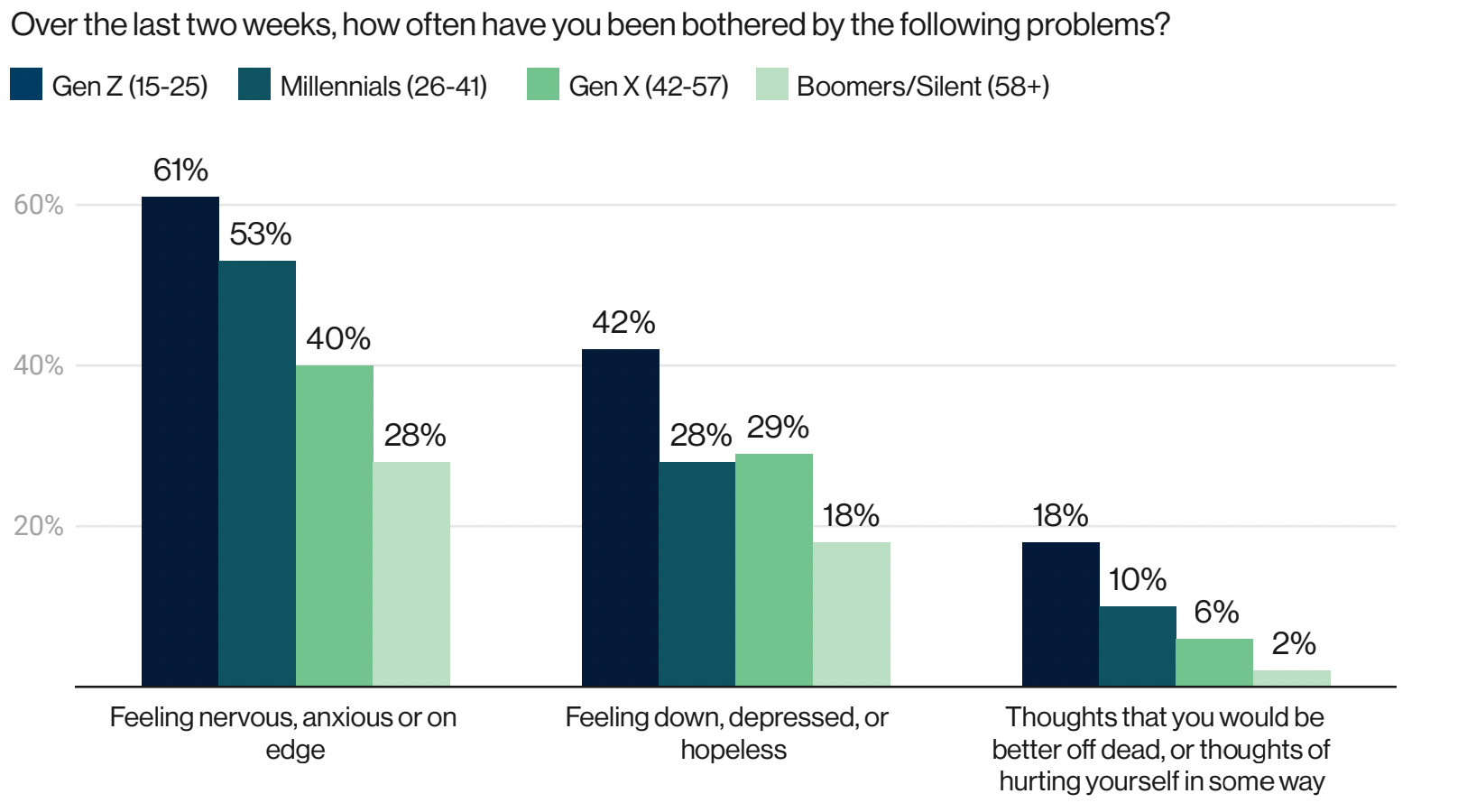
All of these data points indicate that our current approach to psychiatry is not working—unless you view its purpose as being to create a larger and larger market for lifelong consumers of psychiatric medications.
Note: Robert Whitaker, in Anatomy of an Epidemic, makes an excellent case that the psychiatric profession's mass adoption of psychotropic medications worsened rather than improved mental health in the countries where they were deployed. I have also seen this transpire on a smaller scale at a facility (with an excellent reputation for the results it had gotten) that used non-medication approaches for treating mental illness. After it was taken over by medicating psychiatrists, switching to a pharmaceutical model resulted in the patient outcomes there dramatically worsening until the facility eventually had to disband. The dynamic I observed at that facility is a microcosm of much of what I have seen within psychiatry, where many excellent approaches (e.g., therapeutic hypnosis) got pushed out by the money behind the psychiatric drugs.
When I went into medicine, the specialty I felt the most affinity towards was psychiatry (there are many amazing and immensely fascinating things with it), and many of my colleagues thought psychiatry was the specialty that best fit my personality (this often decides what specialties medical students pick). However, I had such deeply held objections to the psychiatric drugs, I simply could not bring myself to spend four years medicating patients during a residency to enter the profession.
Note: there are a variety of effective approaches for dealing with depression. One of the things I have been continually amazed by is how often St. John’s Wort (which is relatively safe and readily available) tends to outperform all of the psychiatric medications on the market—which, to some extent, is one of the best arguments I have ever seen against a free market functioning America given that that herb is almost free. In contrast, over 10 billion dollars is spent on SSRIs annually.
Biological Causes of Mental Illness
Although I disagree with the (disproven) chemical imbalance hypothesis that has been used for decades to market psychiatric medications, in addition to the energetic and spiritual aspects of mental illness (which will be further discussed in future articles), there are a variety of biological causes of mental illness. The widespread lack of awareness of these causes in psychiatry still surprises me since, at least in theory, psychiatrists are doctors tasked with medically addressing the root causes of their patient's illnesses—not just prescribing lots of psychiatric medications.
Some of the common causes include:
•Infections—Lyme disease and toxoplasmosis are the most well-known for doing this (others exist, too), and if you can identify and treat the microbe, significant benefit often occurs.
•Nutritional deficiencies—Many of these exist. B1 and B12 deficiency, particularly in the elderly, are two of common ones (best treated with subcutaneous injections of an aluminum-free preparation). Amino acid deficiencies (most easily addressed with a good amino acid supplement) have a variety of causes (e.g., poor protein consumption or poor digestion of protein in the stomach). They are also common causes of psychiatric issues.
•Trace mineral deficiencies—Many of these exist. Low doses of lithium orotate and, to a lesser extent, normal doses of magnesium orotate or threonate, for example, can be extremely helpful for addressing anxiety.
•Neurotoxic pharmaceuticals—I believe one of the most significant problems with pharmaceuticals is the neurologic damage they cause, which then creates psychiatric effects that are erroneously assumed to cause a gaslighted patient's illness rather than being a symptom of the pharmaceutical injury. I have previously written about two classes of drugs this is frequently observed: statins and the SSRI anti-depressants, but many more cause this as well.
To some extent, this also happens with pharmaceuticals that damage other parts of the body. For example, the heart damage caused by the COVID-19 vaccines frequently causes an anxiety-provoking irregular and accelerated heart rate that is almost always misdiagnosed as being caused by anxiety.
•Impaired circulation to and from the brain—This is most commonly associated with the belligerent (e.g. loss of personal inhibition) personality changes of frontotemporal dementia. Sadly this is also a common side effect of the COVID-19 vaccines, which I previously discussed in relation to the causes of Alzheimer's disease.
•Fluid stagnation throughout the body—when the fluids within the body stagnate, the same is also seen with the emotions (thereby preventing them from freely flowing and leaving you). This is why certain exercises (discussed here) are often so remarkably effective for improving mental health (especially anxiety and depression), and may also be part of why the COVID-19 vaccines (which impair fluid circulation throughout the body) adversely affect mental health.
•Compressions—frequently (especially after a traumatic brain injury), individuals will have parts of their head become slightly compressed. I have seen numerous cases of psychiatric illnesses that began after a traumatic brain injury and persisted until they saw a manual therapist capable (e.g., an experienced cranial sacral therapist) decompressing their skull, and I have also seen less overt emotional difficulties respond similarly. I also often see something similar in the center of the chest (which is where people often feel anxiety). As best as I can tell, this is because more space is created in this area, people often feel as though a weight is off their chest, they have more space to breathe, and the metaphorical walls they feel around them are no longer closing in on them.
•Scars—one school of medicine, neural therapy, believes that many problems arise from hyper-sensitive nerves. If a local anesthetic is applied to those nerves, the nerve reverts to normal when the anesthetic wears off. This issue is most commonly encountered within scars, and the field of neural therapy initially just anesthetized (e.g., with lidocaine) each scar the patient had and then went with continuing to anesthetize the ones that gave improvement. One of the many benefits I have observed from neural therapy were profound improvements in chronic psychiatric issues.
For example, one patient at the VA (who had served in Iraq) had severe PTSD, which resolved after his scars from an IED explosion were injected with lidocaine. In another instance, an early thirties female had chronic burning pain and a variety of psychiatric issues (e.g., anxiety) she had been medicated on for well over a decade. After her scar from a significant injury in childhood was anesthetized with lidocaine, both the pain and the psychiatric issues immediately resolved. As mentioned in this article, I have also seen cases where more advanced neural therapy (aimed at dysfunctional neurons rather than just scars) appeared to have dispersed a fluid clump within the body, and the release of some deep traumatic emotional pattern within them followed this.
•Vagal dysfunction—I believe that one of the most common causes of mental illness in the country, particularly anxiety or irregular heart rates, is vagal dysfunction. The autonomic (automatic) branch of your nervous system has two parts, the sympathetic (fight or flight) and parasympathetic (rest or relax) parts of the nervous system, and each of these counterbalances the other.
Note: one of the most commonly used classes of pharmaceuticals is drugs that "rebalance" the autonomic nervous system by increasing or decreasing sympathetic or parasympathetic activity. An enormous number of drugs on the market do this, although it is highly debatable just how much many of them help their recipients.
Many people believe the root cause of disease in our society is excessive sympathetic nerve activation due to all the stressful situations we encounter. The more significant issue is a lack of parasympathetic nerve function, almost all of which is mediated through the vagal nerve.
Because of the scope of this problem, I have looked at more approaches to improving vagal function. At this point, I believe the primary issue is the vagal nerve being compressed and that having a manual therapist address this compression is the fastest and most effective way to improve vagal function (although many of the other approaches can be helpful to consider once the vagal nerve has been decompressed).
My leading hypothesis for why vagal nerve issues are so common is that the vagus nerve exits your brain at the back of you at the base of your skull. This matters because when we look at screens, we typically bend our necks forward, which puts a lot of strain on the muscles in the back of your neck that keep your head from going too far forward. Our modern behavior thus chronically tightens these muscles which in turn chronically compress the vagus nerve.
In addition to these causes, many others exist as well that I will review in future articles. For example, Chinese Medicine has a remarkable model of mental health that ties many emotions to individual organs rather than the brain and is often very helpful for addressing challenging psychiatric issues.
Integrative Psychiatry
Since there are so many potential approaches to psychiatry, numerous psychiatrists combine integrative medicine with psychiatry and often can get excellent results for their patients. Unfortunately, like other branches of integrative medicine, this type of care is nearly impossible to have covered with insurance and must instead be paid for with cash.
Integrative psychiatry utilizes many different approaches, including the modalities described throughout this article, so it’s not possible for me to synopsize the discipline here. However, I would like to share two examples from functional medicine.
First, minor genetic variations seen in the population are known as SNPs. Numerous SNPs alter psychological behavior (e.g., the COMT SNPs are well-known and associated with anxiety-related personality traits). Many of these SNPs can be addressed with supplement regimens that compensate for the abnormal enzyme functions resulting from the SNPs.
Secondly, I would like to discuss the work of William Walsh, PhD. Walsh spent 20 years building a database of 2,800 depressed individuals (which had over 300,000 analyses of blood and urine) and identified five common patterns that were seen.
Undermethylated depression arises from low activity at serotonin receptors due to rapid re-absorption after serotonin is released into a synapse. This occurred in 38 percent of the patients he studied and is not serotonin deficiency, but an inability to retain the serotonin in the synapse for a necessary amount of time. Patients usually report excellent improvement in mood with SSRIs, but for some, serious side effects such as headache or loss of libido can occur. Nutrient therapy should avoid folates, but use SAMe- methionine. Other nutrients such as zinc, serine, inositol, calcium-magnesium and vitamins A, B6, C, D and E can be supplemented as needed.
Symptoms and traits: Strong willed, tendency toward obsessive-compulsive disorder, calm exterior with high inner tension, competitive and perfectionistic, addictive tendencies, high libido and more than 75 percent exhibit seasonal allergies.
Undermethylated people are the “classic depressives,” according to Walsh. Highly depressed, but typically able to hide it; undermethylation tends to run in families. About 20 percent of babies are undermethylated at birth.
High copper depression is marked by extreme levels of copper in the blood and brain, causing a dopamine deficiency and norepinephrine overload. Increased copper retention is necessary to rapidly produce capillaries and blood vessels for the growing fetus, and some mothers are unable to eliminate the excess copper. Walsh suspects that postpartum depression is usually caused by copper overload. Seventeen percent of the depression patients in the study fit this category. Most reported little effect from taking SSRIs, but gained relief from embarking on nutrient therapy to normalize levels of copper.
Symptoms
and traits: More than 95 percent female with onset during hormonal event,
high anxiety, tendency to panic, estrogen intolerance, tinnitus, sensitive
skin, intolerance to cheap metals.
Pyroluric depression occurs when serotonin production is impaired and there is a high level of oxidative stress. The production of pyrroles/ hydroxyhemopyrrolin can increase with stress, which in turn decreases zinc and B6 – nutrients that are essential for the production of neurotransmitters such as serotonin, melatonin, GABA, and acetylcholine. SSRIs were advantageous for the 15 percent of the patients with pyroluric depression. Nutrient therapy includes normalizing B6 and zinc, adding antioxidants, and augmenting with biotin and primrose oil.
Symptoms and traits: Severe mood swings, extreme anxiety and fears, poor short-term memory and reading disorders, little to no dream recall, sensitivity to light and noise, abnormal fat distribution.
Low-folate depression is of critical importance, in that most of the shooters in some 50 school shootings over the past five decades likely had this type of depression, according to Walsh. For these patients, taking SSRIs can lead to suicidal or homicide ideation. Nutrient therapy using folic acid and vitamin B12 supplements helped patients in the study. For some, anti-anxiety drugs (benzodiazepines) such as Xanax, Valium, Klonopin and Ativan were also beneficial. Twenty percent of the patients in Walsh’s study fell into this category.
Symptoms and traits: High tendency for anxiety and panic, non-competitive in sports and games, food and chemical sensitivities, high musical or artistic ability, underachievement, sleep disorders, absence of inhalant allergies, low libido, tend to be “people persons,” constantly talking.
Toxic metal depression is caused by toxic-metal overload—usually lead poisoning. The removal of lead from paint and gasoline has lowered the frequency of these cases. Walsh estimates that about 5 percent of depressed patients fall into this category. Nutrient therapy concentrates on zinc, glutathione, selenium and other antioxidants – and calcium in the special case of lead poisoning. In severe cases, hospitalization and chelation may be necessary.
Symptoms and traits: Unrelenting depression, abdominal distress, tendency toward irritability and/or anger, absence of trauma or emotional triggers, food sensitivities, metallic taste in mouth, bad breath.
When you read through this, it is almost hard to believe that despite his research being available for decades, virtually no one in psychiatry knows about this, especially since so much of what psychiatrists do is treat depression.
Note: Walsh has made other very insightful discoveries with other common psychiatric disorders. His work can be viewed on his institute’s website and is further discussed in his book Nutrient Power: Heal Your Biochemistry and Heal Your Brain.
Walsh’s work touches upon the much broader discipline of Orthomolecular Psychiatry, a field which has linked nutritional disorders to a wide range of psychiatric disorders (e.g., a niacin deficiency to schizophrenia). I have been draw to this discipline long before I became a doctor, and there are a remarkable number of insights the field has created which unfortunately go far beyond the scope of what I can fit within a single article.
Note: there are also a variety of important aspects of integrative psychiatry such as those which relate avoiding food allergies (e.g., certain food colorings appear to trigger ADD) or balancing and optimizing hormone levels. While I have studied both of these and seen them work, I do not consider them to be my fields of expertise and thus avoided discussing them here.
Conclusion
One of the significant challenges I face with writing this Substack is deciding what to cover at what time (because there is always much more I want to delve into than there is time for). The specific issue of individuals suppressing and withdrawing from emotions kept coming up over and over for different people in my life over the last week, so I took that as a sign it was time to write about it.
On the surface, emotional contractions seem like a very abstract or esoteric concept. Still, once you learn to recognize them, you quickly see how pervasive they are and will wonder how you never saw them before. Initially, one of the best signs of an emotional contraction is if you notice you or someone else blinks exactly in sequence with saying something. This is because blinking is a reflex the body will frequently do when it is internally conflicted about something it is saying (such as when someone say something that deep down they don't actually believe).
Note: The body language community considers blinking not to be a good indicator to use to determine if someone is lying because people also spontaneously blink all the time. However, if you focus on identifying blinks perfectly synchronized with statements, especially if you also "feel" something tightening up concurrently with the blink, they are extremely useful for reading people.
One of the most significant problems in our society is how often people lie to themselves (e.g., they say something they think they "should" say even though their hearts and body conflict with it). Once you train your perception to focus on recognizing emotional contractions, it becomes astounding to see firsthand how pervasive this issue is. When I've reflected on why terrible things (e.g., the Holocaust) tend to happen throughout history, I tend to find they too, are a manifestation of this issue.
More specifically, in many instances where something horrific happens, it does not come out of nowhere. Instead, the evil first transpires on a small scale and gradually grows and grows until it becomes normalized and can be conducted on a horrific scale. In the case of the deadly COVID-19 mandates, we saw this happen in two different ways.
First, most of what was done with them had been done on a smaller scale with many other toxic pharmaceuticals and had become an expected norm not enough people spoke out against prior to COVID-19. Secondly, throughout the entire pandemic, gradually escalating bad policies much of the public disagreed with (e.g., masking then lockdowns or denying safe and effective care for COVID-19 while pushing dangerous hospital protocols) becoming normalized paved the way for the highly unpopular vaccine mandates.
During the escalation period, a large portion of the population can tell what is happening is wrong. However, because it's "difficult" to speak out against the existing narrative, they choose to deny those feelings, close their hearts and minds down, and instead say the safe thing to go along with the crowd's narrative. This emotional contraction is a huge problem, and I strongly believe it is a root cause of many of the terrible things that have happened throughout history.
Since my family suffered through numerous genocides, I have always made a point to note when something I feel is very wrong is happening and then ask if I am choosing to indirectly support it because that's the "easy" thing for me to do. For example, I believe animals have a significant degree of consciousness, and I feel what happens within the processed meat industry (and slaughterhouses) is horrific and something you cannot ethically support. Conversely, I have no issues with people eating humanely raised meat and actually support it because I feel economically supporting those operations is the most effective thing we can do to promote animal welfare.
Whenever I bring up this topic with people who eat factory-farmed meat, I can tell many people essentially feel the same way I do but choose to deny those feelings and close their minds to what is happening because it is "easier." After I watched this dynamic for a few years, I decided I would only ever eat meat I felt was ethically raised, with no exceptions whatsoever, because if I did otherwise, I was willfully engaging in the same conduct I saw create so many different problems throughout history.
Note: Mattias Desmet's theory of "Mass Formation" provides one of the best explanations for what we have all watched transpire throughout the pandemic (best summarized in this remarkable interview with Tucker Carlson). A key point he made was that those deadly dynamics establish themselves in society because those who could speak out against them do not do so. I believe the tendency towards emotional (and mental) contractions detailed throughout this article explains why many people do not do what know deep down is right in those situations.
I sincerely hope you have found this to be a productive topic to explore and that it has left you with an appreciation of the importance of being connected to ourselves and those around us. In this article, the major topics I skipped were sleep and addressing trauma. In the second half of this series, I will delve into both and share the best method I have found for resolving deep psychological issues (which often requires addressing insomnia) and releasing trapped emotions.
The Profound Consequences of Trauma and Insomnia
·
MAY 24

Thank you for your time reading this and your openness to considering the concepts put forward here. I would also like to know if you do or do not appreciate focusing on this area of medicine.
The Forgotten Side of Medicine is a reader-supported publication. To receive new posts and support my work, please consider becoming a free or paid subscriber.
Subscribed
Thank you for reading The Forgotten Side of Medicine. This post is public so feel free to share it.